Episode Summary:
In this episode, oncologist Dr. Bruce Montgomery covers precision cancer diagnosis and targeted therapies, for prostate and other cancers. Thanks to rapid-sequencing technology and medical advances, cancer care is better able to identify specific genetic alterations causing a cancer, and identify a specific therapy targeted against that cancer variant.
Guest:
R. Bruce Montgomery, M.D. Oncologist, Clinical Director of Genitourinary Oncology at the Fred Hutchinson Cancer Center. He is a Professor of Medicine, Oncology and Urology, University of Washington.
During This Episode We Discuss:
- Precision diagnosis and therapy have changed some people’s lives, by adding years and quality to their lives, and avoiding treatments that would not help them. There is still much to be learned and research is ongoing for many cancer types and treatments.
- DNA sequencing looks for both familial markers of cancer risk (such as BRCA markers) as well as specific DNA changes in tumor tissue. For patients diagnosed with cancer, consult with your provider about whether or when you should be tested for specific variants.
- Listen to another podcast episode on precision medicine for more information on this growing trend in health care—Episode 28: Medical Genetics. Original Guide to Men’s Health Podcast
- September is National Prostate Cancer Awareness Month—see our episode on prostate cancer: Episode 10. Prostate Cancer: A) Detection, Diagnosis and PSA, B) Surveillance and Treatments. Original Guide to Men’s Health Podcast
Quotes (Tweetables):
“This is a new pathway in oncology and cancer therapy.”
Dr. Pelman
“And we have made real advances.”
Dr. Pelman
“I think the beautiful part [is] how much easier it has been to do DNA sequencing, among the other things, over the last several years, [which] has allowed us to make huge advances.”
Dr. Montgomery
“We have made huge strides.”
Dr. Pelman
“Oh, night and day, for sure.”
Dr. Montgomery
Recommended Resources:
- U.S. National Comprehensive Cancer Network Guidelines. Click on the Patient Resources tab and then the tab Guidelines for Patients tab, and then click on prostate or other cancer type for more information. This information is compiled and updated by panels of experts.
- FORCE: Facing Hereditary Cancer Empowered. Information and support resource for people who already know they have certain risk variants of genetic or other biomarkers.
- U.S. National Institutes for Health: The Promise of Precision Medicine
- American Cancer Society: information on Precision Medicine
- Episode 28: Medical Genetics. Original Guide to Men’s Health Podcast
- Your healthcare provider, major medical centers with oncology units
Episode Transcript:
Dr. Richard Pelman (00:00):
The Original Guide to Men’s Health is moving to a monthly release schedule. We will be releasing new episodes the first Wednesday of each month. We really appreciate you listening, and we hope you enjoy this episode.
Dr. Richard Pelman (00:18):
Whatever you do, whatever you enjoy, you need your help. Welcome to the Original Guide to Men’s Health, a podcast designed for men of all ages to learn about and access good health. This guide shares knowledge on how to be and stay healthy. Maintenance and prevention strategies along with reviews of conditions and issues affecting wellness are explored. Please join me, your host, Dr. Richard Pelman, as I interview renowned experts who will provide you with timely, relevant, and vital information so that you can embark on a journey towards better health.
Dr. Richard Pelman (01:07):
On this episode of the Original Guide to Men’s Health, we will be reviewing precision oncology. Helping guide us through today’s episode on precision oncology is Dr. Bruce Montgomery. Dr. Montgomery is a board certified oncologist and clinical director of genitourinary oncology at Fred Hutchinson Cancer Center and the University of Washington Medical Center. He is a University of Washington professor of medicine, oncology, and urology. Dr. Montgomery divides his time between seeing patients at the Fred Hutchinson Cancer Center, prostate cancer specialized area, and research. He is a compassionate, conscientious, skillful physician, a real intellectual when it comes to cancer knowledge, and an outstanding researcher who is now devoting a majority of his research time to clinical trials. Dr. Montgomery earned his medical degree at Duke University. He subsequently undertook his internship and residency in internal medicine at the Brigham and Women’s hospital in Boston, Massachusetts, and undertook his hematology-oncology fellowship, medical oncology at the University of Washington. Welcome Dr. Montgomery.
Dr. Bruce Montgomery (02:30):
Dr. Pelman, thank you for having me on. I really appreciate the opportunity to talk to you and to other folks who might be listening.
Dr. Richard Pelman (02:38):
There’s a distinction about precision medicine and precision oncology. So why don’t we first start with exactly what are we talking about with precision oncology. Dr. Montgomery, thank you for joining us.
Dr. Bruce Montgomery (02:52):
So precision oncology is defined in different ways by different people. The way I tend to use it is to say, we use a biomarker to help to tell us whether someone is going to benefit from a therapy or not. And by using that biomarker to say, this is definitely the therapy for you, you’ll get better outcomes, or for you because your tumor has this marker in it, we know that it won’t respond to X, Y, or Z. So the idea being that that’s what’s called a predictive biomarker. So the ability to design therapy based on the presence of this alteration in the cancer. And so from my perspective, that’s the way in which most precision oncology is used. Viewed more broadly it’s essentially saying any biomarker that tells us how to use a therapy could be considered precision oncology. I like to use it attached to a very specific intervention.
Dr. Richard Pelman (03:56):
So you know, our audience may have heard over time, the term moonshot. There were federal funds, we were going to conquer cancer. Dr. Lee Hood, who pioneered a lot of this, talked about P4 medicine. He called it predictive, preventive, personalized, and participatory, and we’ve evolved. This is a new sort of pathway in oncology and cancer therapy. I’m sure that the listener audience is familiar with chemotherapy and the knock against all the chemo was you were dropping an atomic bomb and killing everything. So kind of fill in a little bit about how this is different. You’ve given us a little definition, but let’s keep going there. We’re tailoring therapy.
Dr. Bruce Montgomery (04:40):
The moonshot, as you said, the idea behind that was to be able to find the right therapy for the right person at the right time. The idea is that mostly what we’re talking about in medical oncology these days is doing largely what’s called DNA sequencing, meaning taking the cancer, pulling it apart, looking for alterations that have occurred in the process of development or evolution of the cancer that then make it hopefully more sensitive to very specific therapies, and in the best situation, the therapy is specifically targeting the pathway that is altered. So that’s, you know, sort of the most intelligent engineering of how to treat somebody. And by doing that, you hopefully minimize side effects and you optimize outcomes. So that was the whole idea behind the moonshot. So what we do in medical oncology in general is that in patients who have specific malignancies, most of the time, we’re looking for very specific targets.
Dr. Bruce Montgomery (05:48):
Some people would argue that every patient with an advanced malignancy should have DNA sequencing done. And there are other people who say that doing any DNA sequencing of any kind is largely irrelevant because it hasn’t been shown to improve outcomes. I would say the truth probably lies somewhere in between. That is, from my perspective, there’s no question that patients who are dealing with some specific malignancies, if we can find an alteration to which we can match a therapy, those folks benefit. Not only do they have their cancers respond, but they live longer and their quality of life is better. And so I’m happy to talk about specifics. I obviously tend to think more about prostate cancer than anything else, because that’s our most common disease that we treat. But, you know, there are many areas that have been, there have been incredible advances made. So for example, when advanced lung cancer, you know, back in the day, what we did was we used platinum chemotherapy to treat everybody. Now, most people who present with an advanced non-small cell lung cancer will have sequencing done. And in some cases, therapy is designed specifically around the alterations that are found in the tumor.
Dr. Richard Pelman (07:07):
Let’s go back a little bit. We’re talking about sequencing. DNA sequencing. Are we talking about somebody’s DNA that you would get for 23-and-Me, or are we looking at the tumor DNA, or are we talking about both?
Dr. Bruce Montgomery (07:21):
The short answer is both for a couple of different reasons. At its simplest, you sequence the tumor DNA and you try to find alterations that are specific to the cancer. The truth is that in a fair number of people, their normal DNA also contains alterations that tell us why the cancer developed. So for example, folks who inherited an alteration, BRCA1 or BRCA2, when you sequence the tumor, you’re also sequencing the normal DNA as well. And the idea is that you pick that up along the way. The important thing is when we’re doing those sorts of tests on tumor DNA alone, it’s important to recognize those folks who did inherit one of those alterations, because that has implications for family. So the short answer is, for many people, sequencing both the normal DNA, what’s called germline DNA, and the tumor DNA, which is called somatic DNA, both of those are important things to think about when we’re talking about trying to find the right therapy.
Dr. Richard Pelman (08:26):
And when we talk about therapy, most people are familiar with treating cancer with chemotherapy. Is this always just going to be applied to chemo or are there other forms of therapy that this is useful?
Dr. Bruce Montgomery (08:38):
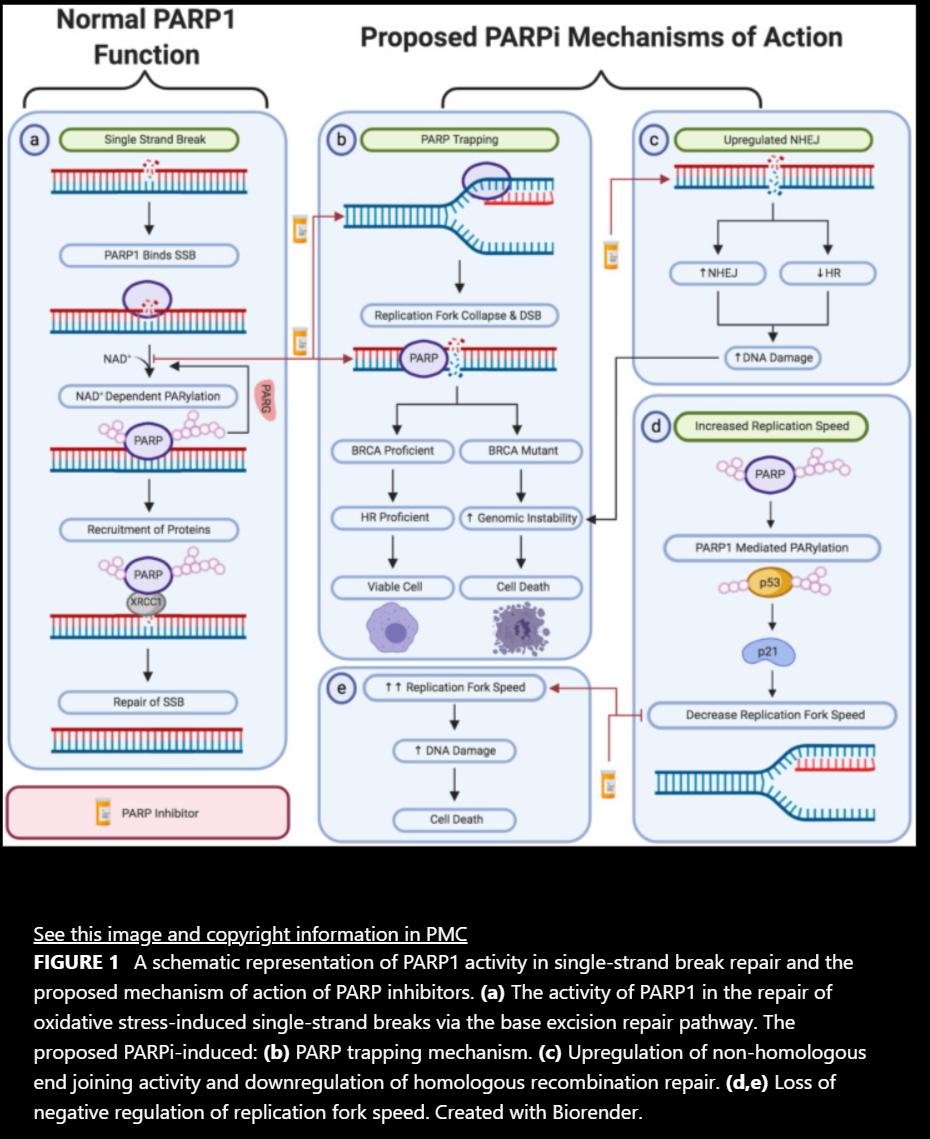
Actually, there are some types of chemotherapy that essentially are targeted therapy. So for example, cancers that contain these BRCA alterations, which are very common in breast, ovarian, pancreatic, and some prostate cancers, platinum-based chemotherapy can be exceptionally effective in those patients. On the other hand, other drugs also target those alterations. So things like, what are called PARP inhibitors, poly ADP ribose polymerase. So those are drugs that are pills that sort of block one of the pathways that the cancer uses to survive despite the fact that it has a tough time repairing DNA damage. And those PARP inhibitors can be exceptionally effective. There are also what are called tyrosine kinase inhibitors. If you think about it very generally, those are like chemotherapy, but they are targeting very specific proteins that are signaling along these pathways that are responsible for cancer, that in many cases can be really, really effective.
Dr. Richard Pelman (09:40):
And you mentioned BRCA, breaking that down for people listening who may not be familiar with it. It was one of the early determinants for breast. Dr. Mary Claire King of the University of Washington found that gene. So just elucidate a little bit more about BRCA.
Dr. Bruce Montgomery (09:59):
As you said, Dr. King was one of the very first people who recognized that there were women who were developing breast cancer at a very early age and there tended to be a pattern of that in the family. She went back, took the DNA from these families, and specifically found that in a subset of folks, there were alterations in this gene that, BRCA sort of stands for breast cancer gene one is what the original gene that they found was. Subsequently there was another gene found involved, and they’re both involved in repairing DNA damage to cells, something called BRCA2. Both of those are genes which, when they’re inherited by somebody, particularly women, but also men, carry an increased risk of some very specific cancers like breast cancer, ovarian cancer, male breast cancer, in fact, prostate cancer. And that’s a very important risk of developing significant prostate cancer down the road.
Dr. Bruce Montgomery (11:01):
Those again are part of what’s called DNA repair. So your body has evolved this process of being able to repair DNA damage because damaging DNA is the first step to getting cancer. Your body obviously doesn’t want to get cancer that takes you off the road of life. So these genes are involved in repairing that damage from the sun or what you eat or whatever. The issue is if you inherit one of these genes that doesn’t work all that well, then parts of your body are more susceptible to actually developing full blown cancer because it can’t repair that damage that we all sustain just walking around every day. So that is one of the best defined predispositions to developing cancer. Those alterations, it turns out, can make cancers extremely susceptible to targeted therapies like the PARP inhibitors, some platinum agents, and a few other therapies as well.
Dr. Richard Pelman (11:57):
This is your body’s surveillance system. I’ve always been under the impression that as we age, our surveillance system gets weaker and sometimes just can’t do the repairs like it used to, but there’s obviously some genetic predispositions towards this as well.
Dr. Bruce Montgomery (12:12):
Absolutely. And as we age, we tend to build up DNA damage and the system for repairing that damage also is not as effective. So you’re absolutely right. That is some part of normal aging. But as I said before, you know, if people don’t have a good repair system from the very beginning, they can develop cancer at a much earlier age.
Dr. Richard Pelman (12:33):
So we spoke a little bit about some vocabulary issues that we’ll be referring to, the difference between somatic and germline. So testing the tumor itself is again called somatic testing. And then when you just get your blood drawn and you look at your DNA, that’s germline.
Dr. Bruce Montgomery (12:52):
Yeah. It’s just the DNA that you inherited. You know, every chromosome has half from your dad and half from your mom. So you inherit two of those genes. And if you inherit an alteration from one of them, half of your capacity for repairing DNA in all your cells really is compromised. So that’s why looking at germline DNA sometimes tells us a lot about the cancer.
Dr. Richard Pelman (13:15):
We spoke a little bit about this in the genetics episode that we did, but I’m sure listeners are going well, should I go out to 23-and-Me and have my germline sequence? Should I have my blood drawn and look for something that makes me susceptible?
Dr. Bruce Montgomery (13:32):
Some of these sort of vendor products that you don’t have to go to a doctor to get like 23-and-Me, some of them do include genes that are involved in things like DNA repair. The issue is that they only test a couple of different alterations in those genes. Whereas a dedicated genetic test looks much more deeply and much more completely at those genes and really means something. The main reason I bring that up is that because somebody has done 23-and-Me, that doesn’t necessarily give you a complete answer one way or the other. I would say, I don’t think that testing your normal DNA for a cancer predisposition makes sense for everybody, for sure, because there are all these alterations in those genes that don’t mean anything. We have very specific guidelines and the guidelines change as we do more research and find more alterations that mean something to people.
Dr. Bruce Montgomery (14:28):
But, you know, for example, in folks dealing with prostate cancer, it’s a very clear recommendation that folks who are dealing with disease that’s gotten out of the prostate, metastasize is what they call it, those men are people who definitely should have germline testing done because that can, you know, help them to find other treatment options and its important for their family if they in fact inherited something. So the short answer is absolutely the right thing for some people, not the right thing for everybody to go doing, and certainly not to go doing and the wrong.
Dr. Richard Pelman (15:03):
And for more information, I’ll just refer listeners to the episode on genetics with Dr. Jarvik. It really did give us some background as to what’s available and what’s not. And there is a national effort if you’re accepted that will do your DNA screening. It’s a national program, but listen to that episode. So going back to tumors, I’m going to hold off for a second as far as specifics of what kind of cancers and just look at what kind of testing is actually being done. That category of all right, you’ve got a tumor, we’re going to do this somatic testing. What happens? What are we actually looking at?
Dr. Bruce Montgomery (15:42):
The first thing is you have to decide which tissue to test. You know, you’re taking tissue of some kind and the right tissue to test depends on what the setting is. So in some people it’s taking a diagnostic biopsy, the tumor tissue that’s taken at the very first time a diagnosis is made, that tissue is sent off. You can either send off the, there’s something called a block of tissue that has the tumor tissue put into wax, and then it’s cut and you can actually send the block itself, or just pieces of the tumor tissue that are cut off onto a slide that is usually sent to what’s called a vendor, a company that does the sequencing, the majority of the time. And what they do is they take that stuff off the slide or out of the block, they break down what’s in that tissue sample, and then they sequence all the nucleotides in that sample, looking at very specific parts of the DNA.
Dr. Bruce Montgomery (16:35):
They don’t sequence the whole DNA, and there’s lots and lots of DNA in there, but we really are looking specifically at genes that we know mean something. And so that is usually done over the course of several weeks. You know, sometimes the results can come back very quickly within less than a week, but the majority of the time, that takes somewhere between two and four weeks and then the report comes back to the provider that says, we found these genes that are altered. The alterations have this implication. And hopefully something can be found that can be a benefit to people. And, you know, again, for the right person, doing that testing makes sense. I want to reemphasize before we go further. Not every single person with advanced malignancy is expected to be able to find something. So I don’t think that necessarily, you know, although there’s this propensity for all of us to, you know, more information is always better for a lot of people doing that, sequencing doesn’t really provide any information because we haven’t ever found a mutation in that type of cancer that’s ever been able to be used to treat them differently. Definitely is part of research we do all that, but not necessarily as part of clinical care.
Dr. Richard Pelman (17:59):
So along that direction, and then I’ll go back to next generation sequencing for you to elucidate a bit about that, but in the Emperor of all Maladies, which I think was a wonderful book, one of the greatest treatments that came along came because a researcher happened to be attending a meeting and heard somebody speak and told a colleague that they should meet. It was almost happenstance. And, you know, somebody says, well, how do they know that there’s nothing that works for this tumor? How does my oncologist know? We are now networked into work groups so that the information is shared much more readily and that somebody on the east coast is getting information from the west coast and from the midwest. Yes. I mean, just let people know how this works in this day and age rather than happenstance.
Dr. Bruce Montgomery (18:43):
Right. So great points. I think, as we all know in the midst of this pandemic, virtual communication has been critical. We all tend to communicate with each other about new research because that’s obviously the cutting edge. That’s what we’re all trying to find, the newest, greatest thing for the patients we see. That communication takes place through a number of different media and mechanisms. So, you know, publication of journal articles is out there. The vast majority of journals now are electronic. You can access them immediately from anywhere. So publication of those results is critical. We have meetings, they used to be face-to-face and hopefully we’ll get back to that soon, but you know, virtual meetings now many times per year. Some of them are subspecialty meetings where the newest, greatest research is being presented. Thousands of people will attend these meetings to see the latest data that’s come out of either both clinical trials and in and out of the laboratory that informs the subsequent clinical trials. And then the companies that are involved in doing this research are, both the sequencing and the clinical trials, are just as invested in making sure that everybody knows the results as quickly as possible as all the rest of us are. I would say in this modern age, communication happens so much faster than it used to, and access to the information that can inform the next experiment or the next clinical study or the next treatment is generally much more available than it used to be.
Dr. Richard Pelman (20:19):
And going back to next generation sequencing, or NGS, review that it’s targeted and some comments about whether it’s the whole exome or the whole genome, just review that and break it down a little bit.
Dr. Bruce Montgomery (20:35):
We talked about DNA sequencing and the issue is that sequencing all the DNA and somebody’s tumor, or even just in their normal DNA, there’s a lot of DNA in there that has no impact on things like cancer therapy. So to sequence all of that, it’s called Whole Genome Sequencing. That is literally sequencing every nucleotide in somebody’s genome. And then there’s, what’s called Whole Exome, which means just sequencing the part of the DNA that ends up being made into protein, because that’s actually what the majority of us are all ourselves made out of, is proteins. And so that’s more important. But what’s called targeted next generation, so NGS or next generation sequencing, is just the method of very rapidly sequencing DNA very efficiently. What targeted means is that the majority of the time what happens is a company or an investigator just says, okay, these are the genes that mean something for therapy or for predicting response to something more how people are going to do. We’re going to sequence that. In most cases, the sequencing is being done many, many times to make sure that it’s accurate and that the result is what we think it is. So we take most cases, maybe 50 genes when we’re talking about germline testing, or hundreds of genes when we’re talking about sequencing the tumor DNA, or somatic testing and sequencing them many, many times to get the answers about what we can find.
Dr. Richard Pelman (22:03):
And is that currently the most popular platform or are there other ways of achieving this?
Dr. Bruce Montgomery (22:10):
From a research standpoint, a lot of people are doing the broader sequencing effort. There are other tests for biomarkers that aren’t DNA. So for example, in prostate cancer, there is an RNA test looking for a very specific type of receptor for testosterone called the androgen receptor. There are these variants of the androgen receptor, which are sort of hyperactivated. And the way to detect them is by pulling RNA out of cells that are floating around in the bloodstream. So, you know, there are a broad range of different ways of looking for this for these sorts of biomarkers. The DNA sequencing, again, targeted DNA sequencing that we were talking about is, far and away the most popular and the one that has the most of the drugs attached to it. But there are a range of other approaches as well.
Dr. Richard Pelman (23:02):
So the upshot of course is looking at who should be tested. And maybe we will now kind of talk about some examples because this episode will be launched in September, which is prostate cancer awareness month. And you know a lot about prostate cancer. Let’s start there. So a patient or somebody who’s listening who knows somebody who has prostate cancer says oh, you have to listen to this episode, you should go get tested. We talked about prostate cancer generally after diagnosis of being clinically localized or metastatic. And certainly there are people we feel are localized, but sometimes there’s microscopic disease that’s already escaped based on certain risk factors. How high their PSA is and the grade of the tumor. So somebody has been diagnosed with prostate cancer. Who should go out and have their tumor examined or their blood examined.
Dr. Bruce Montgomery (23:58):
So the majority of the utility of doing sequencing of the tumor is for folks who have disease that’s clearly out of the prostate because for those folks there are drugs that are either available for use today, or they will be, when they reach the point where that becomes necessary. There are folks who have localized prostate cancer for whom doing that sequencing might be useful. So for example, there are folks who, as I think you know better than anybody because you’re in urology, we’ve sort of moved some of the tendency to treat everybody to this idea that people can just watch their cancer if it’s not really an immediate risk to them. And that’s what’s called active surveillance. That’s an inappropriate approach. I’m sure you’ve had other folks on talking about this for men who have small volume, low grade cancers that aren’t predicted to have a big impact on their outcomes for a long time.
Dr. Bruce Montgomery (24:57):
We know that for example, men who have inherited one of these alterations in genes like BRCA 1 or 2 are at higher risk for developing advanced prostate cancer. Cancer that gets out of the prostate and becomes the thing that threatens them. So what’s an area of very active discussion and research right now is, are people who are germline carriers of these alterations, like BRCA 2, are those men who really are appropriate for active surveillance? I think there are folks that come down on both sides of that discussion, but I think certainly many providers who are considering putting men on active surveillance are looking at whether they inherited one of these alterations because from the data that we have, we know that their risk of having something happen that we don’t want is higher. So that would be one situation.
Dr. Bruce Montgomery (25:55):
Okay. The other situation for getting sequencing, although the national guidelines say that people who have high risk cancer are appropriate for sequencing, I honestly don’t necessarily do that for the majority of men who have disease that can be treated with radiation or surgery because there isn’t anything we can do with those results for those men right now. And, you know, you want to have the most up-to-date information when it’s relevant for somebody down the road. So I think every man with metastatic prostate cancer should have both the germline tested, meaning the normal DNA, to look for whether they inherited that alteration, or somatic sequencing. And that can be either their prostatectomy specimen, if it’s still around, or it can be even a metastasis biopsy. That’s actually how we originally found all these alterations in prostate cancer. Or there’s something called circulating tumor DNA, where you can actually just draw blood and you can pick up DNA fragments that are floating around in the bloodstream that the tumor has shed and can give you a good sense of what’s going on with cancer in real time. And it’s pretty easy to access and generally a very good approach.
Dr. Richard Pelman (27:08):
So a patient who is clinically localized, and we talked about guidelines, I suspect you’re talking about the National Comprehensive Cancer Network guidelines, which nccn.org patients can find. And if you’re looking at prostate cancer, you go to guidelines for patients, if you find the header under nccn.org and you find guidelines for patients, and then you’ll see basically every cancer. And if you click on prostate cancer, it’s interpretable. You can follow it. And it comes up as a nice little booklet and you can read it. The NCCN guidelines that are not for patients are a little more in depth and that’s for practitioners, but that’s where we get this information.
Dr. Bruce Montgomery (27:53):
Exactly. Those are expert panels who take all the data into consideration. And sometimes part of it is opinion. That’s part of being an expert, right? As the people who do most of the research and do the clinical trials, you know, they generally have the best sense of how both treatment recommendations and evaluations should be done. So that NCCN is a great resource, as you said.
Dr. Richard Pelman (28:19):
And then somebody who’s category of tumor is more active or their PSA is higher. The volume of tumor is larger, who should move ahead with treatment and not be in surveillance. We would hope they’re clinically localized. We look for any metastatic disease. It’s not there. They move ahead with either radiation or surgery, which are the two main modalities at this point. They don’t have to worry though that if, you know, there is residual tumor somewhere that was hiding that they didn’t have it sequenced initially, because, as you said, it can be from the paraffin block that’s stored, so you can always go back, or from the actual metastasis should that develope.
Dr. Bruce Montgomery (28:59):
Exactly. And we just did some work, not very long ago. One of my colleagues, Dr. Schweitzer and I, and a number of other folks, we went back and we looked at the tumor tissue that was taken at the very beginning, either prostate needle biopsy or the prostatectomy specimen. And, you in folks who had had one of these targetable alterations defined from things like metastasis, we actually show that they agree the vast majority of the time. So it’s very reasonable to sequence the prostatectomy specimen or the prostate needle biopsy. If people don’t have other easy ways of analyzing tissue.
Dr. Richard Pelman (29:36):
In some instances where there’s been radiation, can the radiation change the character of tumor and the metastatic disease?
Dr. Bruce Montgomery (29:43):
With regards to the kind of mutations that we think of, at least as of today, that give people different treatment options. There isn’t actually a lot of data that radiation generates those alterations. And therefore you would miss that from the biopsy that preceded the radiation. And there are some things that happen over the course of treatment pressure from hormone therapies and chemotherapy, and those sorts of things, those alterations can evolve. But most of them are not things that we can necessarily use today to treat somebody differently. So even though they might be, they might be different knowing that those are different, doesn’t change things. So, you know, knowledge is knowledge for sure. On the other hand, what you want to know about is something that you can use to treat somebody.
Dr. Richard Pelman (30:32):
And we have made real advances.
Dr. Bruce Montgomery (30:35):
Oh my God. Yeah. I mean, I think that, you know, the beautiful part about how much easier it has been to do DNA sequencing among the other things over the last several years has allowed us to make huge advances. I mean when I started in this world, and a little younger than you, not by much, the idea is that we just didn’t have options. And then as options came, we treated everybody exactly the same every time. And we are, thank God, evolving out of that approach to one where we can more appropriately personalized therapy for people. And, you know, the research has really been, what’s made that possible.
Dr. Richard Pelman (31:18):
There continues to be research. You know, this is ongoing everyday.
Dr. Bruce Montgomery (31:22):
There are many, many people thinking about this every day, trying to find the next great thing. And many people are very focused on the next great thing. That’s going to be curative for people who have advanced disease. So the good news is that we continue to improve therapy for men who have disease. That’s just in the prostate. We’ve also made some huge strides in dealing with more advanced disease and people are working everyday too, and continue to move forward on that.
Dr. Richard Pelman (31:52):
And just for someone who’s listening, who either has advanced prostate cancer, that’s metastasized or knows somebody who does, say their tumor get sequenced, are they still being treated initially for the metastatic disease, with the first-line therapy, which has been to deprive the tumor of male hormone, or are we moving into this very specialized approach?
Dr. Bruce Montgomery (32:18):
First, as of today, outside of research studies, hormone therapy remains the backbone of therapy for men. And, you know, I know that that’s something that’s been around for many, many years. On the other hand, what we’ve learned is that by doubling down on that, by even more significantly suppressing the signaling through the hormone axis, we’ve been able to add years to men’s lives by adding other drugs right upfront. And now what’s actually happening in the research area is adding these targeted therapies to that combination in men who have just been diagnosed with advanced disease and, you know, looking at whether, you know, when we talked about a little bit earlier, these PARP inhibitors, which were these ways of really leveraging the inability of the cancer to repair DNA damage, we’re looking at moving that into that area. And I know that there are studies being done looking at using those drugs for men whose PSA is just rising. And it actually, even before things like surgery.
*PARP1 possesses Poly (ADP-ribose) activity and when activated by DNA damage, adds branched PAR chains to facilitate the recruitment of other repair proteins to promote the repair of DNA single-strand breaks. PARP inhibitors (PARPi) were the first approved cancer drugs that specifically targeted the DNA damage response in BRCA1/2 mutated breast and ovarian cancers. Since then, there has been significant advances in our understanding of the mechanisms behind sensitization of tumors to PARP inhibitors and expansion of the use of PARPi to treat several other cancer types.
[Image Source:PARP Inhibitors: Clinical Relevance, Mechanisms of Action and Tumor Resistance – PubMed (nih.gov)]
Dr. Richard Pelman (33:25):
Going back to a initial screening, we talked about BRCA. How does an individual who’s listening know if their mother or sister had breast cancer or ovarian cancer, is it a clue that they should perhaps consider getting tested?
Dr. Bruce Montgomery (33:39):
Family history. Although it isn’t completely predictive of whether people carry one of these alterations, you know, a family history of breast, ovarian, pancreatic, or prostate cancer in multiple members of the family. But particularly at younger ages would be reasons for people to be thinking, “oh, you know, I’ve always worried about this. And you know, now maybe I should talk to my doctor about it,” whether in fact, this is a reason to do that kind of testing. You know, it’s important to bring these things up. You know, doctors are obviously trying to do the right thing, but a lot of appointments are 15 minutes and, you know, you gotta get through the things that you’re thinking about that day. You know, bringing that up when you talk to your doctor is really critical. So thanks for bringing that up.
Dr. Richard Pelman (34:24):
And then populations that are at risk that come to mind.
Dr. Bruce Montgomery (34:28):
Yeah. So, you know, in terms of germline alterations, beyond the family history part, we know that for example, black or African-American men are at higher risk for significant prostate cancer. As of today, we don’t seem to see a significant increase in these germline alterations. In general, the frequency is about the same in the Caucasian population versus other ethnic groups. You know, folks who have an Ashkenazi Jewish background are much higher likelihood of carrying one of these alterations and that something is you should definitely pay attention to that. But I think a lot of the time, it’s a matter of asking if there is a family history, seeing if somebody has been tested, sometimes that information actually hasn’t been passed on. And there is somebody who family who actually knows that there is an alteration, but, you know, for whatever reason that information didn’t make it.
Dr. Richard Pelman (35:27):
Again, genetic counselors are available at most major centers. I’ll again, refer people back to our episode on genetics and genetic testing, looking at cancers besides prostate and lung, we spoke a bit about adenocarcinoma. But, for somebody who’s listening who has lung, or knows somebody with lung cancer, let’s delve into that a little bit.
Dr. Bruce Montgomery (35:48):
I think a lot of the era of molecular medicine or precision oncology started when people recognize that in a subset of adenocarcinoma in the lung, there were these… and I’m going to start using terminology that mean a lot, but epidermal growth factor receptors. There are these proteins that were mutated and they discovered them because, you know, there were people who had never smoked and, you know, were getting diagnosed at a young age and they recognized that these alterations were present in the tumor. And then because they knew about these mutations, they developed very specific therapies that target that mutation in those tumors in a way that can be extraordinarily effective. And we’ve continued to develop more and more effective drugs for that. Once they actually discovered that these what are called ETFR mutations existed, then they started looking for other mutations, have found a plethora of these mutations that are not very common, but when you start adding up, how many of them there are, and many of them have these targeted therapies attached to them, which can be extraordinarily effective. You know, it has become really the best. Now precision oncology can change people’s lives because folks who otherwise would have gotten platinum chemotherapy and had a relatively poor outcomes, are now living many years.
Dr. Richard Pelman (37:15):
So as we look at these tumors and the interpretation of these issues, let’s elucidate a little bit more about the findings.
Dr. Bruce Montgomery (37:25):
What usually happens is the tumors get sent off, or the circulating tumor DNA sample gets sent off, and a report comes back to a provider and it says these genes were altered and there are these treatments attached to them. So there are a couple of different aspects to that that are really important for making sure that the provider has thought about, you know, is this something of significance? So first, you know, they need to look at whether that alteration it’s definitely obviously there, the question is, is that something that the patient could have inherited? So being able to tell from the report that somebody might’ve actually gotten that alteration because they inherited it, that is sometimes not very clearly spelled out, but sometimes it is. And it’s sometimes on page 25 of a 25 page report. So one thing is, you know, as somebody who’s interacting with a provider who just interpreted that result, you know, making sure that the provider thought about whether that alteration was something that may or may not have been inherited.
Dr. Bruce Montgomery (38:32):
So that’s one part. The second part is that even this, what is called the circulating tumor DNA, also called the liquid biopsy, which is just a blood draw where we can, again, sort of get the tumor DNA just by doing that simple procedure. The issue is that there is something that is not as widely recognized as I think should be recognized. There’s something called Clonal Hematopoiesis of Indeterminate Potential. That is a mouthful. So we call it CHIP. But what it means is that as we age and our bodies absorb that DNA damage that you would actually referring to earlier, our bone marrow function can sometimes not be normal, meaning that some little collections of cells in your bone marrow start to not make perfect cells, shall we say there are mutations in ’em and the bone marrow isn’t functioning? Well, it doesn’t mean you’re necessarily getting leukemia.
Dr Montogmery (39:31):
We can find these what are called CHIP clones floating around in 10 to 20% of people by the age of seven. Okay. So a good portion of us at the age of 70, have these things floating around. And the thing is some of these alterations happen in genes that are picked up as being something from cancer. And so what happens is this is a very common problem. So for example, again, back to prostate cancer, if we look at a set of patients who had one of these liquid biopsies done, and an alteration was found in a DNA repair gene, for which they might be a candidate for, let’s say one of these PARP inhibitors, almost 50% of those alterations are actually not from the cancer they’re from this CHIP clone. Okay. So the issue is it’s an under-recognized problem that both the provider and being an advocate for yourself, because, you know, saying, and I know this is asking a lot of people, but they should just be aware of it, you know, asking the provider, because if they’re giving somebody therapy based on this alteration, in the tumor, in the report, half the time, it’s not going to do anything to fight the cancer, and it can be expensive.
Dr. Bruce Montgomery (40:50):
People are being exposed to side effects of therapies that don’t work, and then it’s delaying treatment that could work. So that would, I want to comment about that.
Dr. Richard Pelman (41:00):
Is there a more specific way to find out if it’s actually involved in the tumor?
Dr. Bruce Montgomery (41:04):
Yeah. So the best way to do that is having it done through an assay that does comparison of the tumor DNA to the normal DNA from the blood draw. If some labs can in fact get both of those out of the blood draw, just out of the blood draw that was used to get that read, not to tout our own work, but for example, the lab at the University of Washington, which is a commercial lab, they do that tumor normal sequencing. It’s doing both at the same time. And that way you can tell whether it is in fact related to the cancer or not. You can tell sometimes from just looking at the report carefully, for example, if the tumor DNA amount is very high and the amount of this alteration is very low, that really tells you that it’s not from the cancer, but from one of these CHIP clones.
Dr. Richard Pelman (41:58):
And sure somebody is thinking that well, if they find these alterations before I have cancer, can’t they fix it?
Dr. Bruce Montgomery (42:05):
We do know that if we find this CHIP abnormality in someone, their risk of developing, not every cancer, but specific cancers like leukemia is elevated, but because the frequency of leukemia is very low, even though the risk is elevated, if it were found, I think your provider would want to look at, for example, other blood counts to make sure that your other blood counts are normal, if they are, and you’re otherwise doing fine. Although again, the reason you’d be getting this sequencing done most of the time is because you’re dealing with a malignancy of some kind. But if there’s no evidence that the bone marrow function is being compromised, all you would do is just follow that without actually doing any intervention.
Dr Pelamn (42:51):
Just going back to generalities, then people are wondering, well, can they cure something preventively by fixing the gene?
Dr. Bruce Montgomery (43:00):
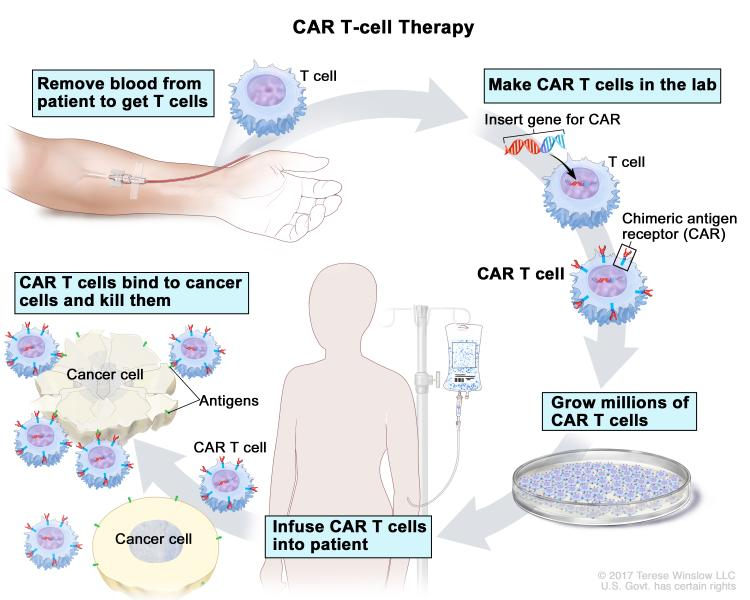
Yeah, that is clearly what all of us want to be able to do. So I think for example, there are diseases that are now being treated by using what’s called CRISPR* technology, where you can in fact insert or alter genetic material in a way that allows you to restore function. For example, either in bone marrow cells, for folks who are dealing with various types of LCME or sickle cell disease and a number of other diseases, although most of them are not related to cancer right now, I think to a degree, some of these approaches that we’re coming to are not that far away from what we did with what is called CAR-T cell therapy, where we basically take somebody cells out and we put constructs into their T cells. So that were hyperactive in their immune system against whatever cancer they’re dealing with, mostly leukemias, and that can be curative and Hodgkin’s disease and various types of lymphoma.
Biologist Explains One Concept in 5 Levels of Difficulty – CRISPR | WIRED
Dr. Bruce Montgomery (44:10):
That has been a huge step in the direction of finding a cure for people with those diseases. Everyone wants to find a way to make immunotherapy more effective because so far that has been sort of the realization of the hope for cure, for people who are dealing with advanced disease right now, solid tumors beyond things like lymphoma and leukemia. We’re still making progress, but we’re not there yet. Let’s just say so far as immunotherapy goes. Now, I would say a very important aspect of this molecular medicine. Precision oncology part is finding folks who have these cancers that are what are called hyper mutated or mismatch repair deficient. They’re not very common, but if by doing the sequencing that is found that immunotherapy can be curative in those people. And that actually is another aspect of this precision oncology effort that can in fact mean a great deal to people. So, but again, it’s just a different way of leveraging immunotherapy for the most important outcome, if possible, which is to cure the disease.
Dr. Richard Pelman(45:23):
And we’ve touched on prostate and lung, but there obviously are a number of other cancers and it would be beyond the time that we have to delve into all of them, but all other cancers are being looked at.
Dr. Bruce Montgomery (45:38):
Absolutely. So, even though, as I said at the beginning, I don’t think that necessarily everybody with every advanced malignancy should have sequencing done. I know because I work with, you know, very smart people over at the Fred Hutchinson Cancer Center, looking at all those diseases that they’re trying to find new targets, new alterations in those malignancies that will be targetable in the near term as we speak. So the research goes on, but many malignancies, you know, it is standard of care to perform this sort of sequencing to find alterations and, you know, asking your provider, if you’re dealing with an advanced cancer, whether that’s the thing to do, if it hasn’t been done, you know, no downside to asking. And I think for many people, it is the right thing. It’s just a matter of the right time. Right.
Dr. Richard Pelman (46:30):
Right and then among your own colleagues and other national centers for somebody who’s listening, who may not be in Seattle and maybe somewhere else, most major medical centers have major oncology centers or cancer centers. And when is it appropriate to go to a very particular center?
Dr. Bruce Montgomery (46:51):
You know, I think sort of across the spectrum of malignancy, one thing I would say is that, you know, if you’re dealing with a significant cancer that hasn’t necessarily gotten out of where it started, but you don’t feel like the expertise in where you are is necessarily what it might be getting a second opinion, seeing a multidisciplinary care team at a medical center that has that expertise is always a good idea. You may not necessarily have to get your therapy there, but the plan for treatment can oftentimes be developed by review of the pathology, the images that have been taken, those sorts of things. So even at the very onset of the disease being seen at a major medical center, if you have something that isn’t, that straightforward is always a good idea from my perspective. And I hope that isn’t too self-serving I think in terms of, you know, taking advantage of the research, that’s taking place at some of these major medical centers, you know, I think when people are dealing with an advanced malignancy, so metastatic anything, getting an opinion, again, you don’t have to make the decision to be treated there, but knowing what your options are and establishing a communication with a provider at one of those centers, so that it may not be the right time now to engage in participation in research, or even just standard of care there, particularly if you live a long distance away, but somewhere along the way, it may be important for you.
Dr Montomery(48:27):
And particularly if you want to take advantage of research and having a contact and having being a known entity within one of those medical centers and only play to your advantage because the research is where the new therapies are coming from and the significant advances are coming from.
Dr. Richard Pelman (48:45):
Right. Are you doing any of this through telemedicine/telehealth?
Dr. Bruce Montgomery (48:49):
So actually a lot of the multidisciplinary care is taking place through what’s called telehealth, as you said. So we are in fact, for example, at the University and the Hutchinson, our bladder multidisciplinary clinic offers distance consults and doing that through the pandemic. And we’ll continue to do that after the pandemic. And, you know, things are a little bit in flux right now about which states will allow us to do telehealth that aren’t the state of Washington, but within the state telehealth consultation is being done much more commonly. And it obviously is much easier. And you can establish whether there’s, you know, a great treatment option or a treatment that hadn’t been considered that could be available to you locally by having one of those consultations. So thanks for pointing that out. That is definitely something that now and going forward will definitely be a boon for folks who aren’t living in New York City you’re in Seattle or Houston, for example.
Dr. Richard Pelman (49:51):
Yeah. Just information for listeners. The pandemic allowed us to resolve or lift some of the restrictions on telemedicine, telehealth for the benefit of patients during the pandemic. And we’d like to continue a lot of those so that there are no restrictions. And that’s currently legislation both statewide and national that’s being looked at well. I always like to wrap up with resources. We talked about the National Comprehensive Cancer Network, other resources that come to mind that you could recommend to people?
Dr Montogmery (50:23):
I think there are a couple. So one is for people who are carriers of one of these alterations, there are organizations out there that are specifically for you. So another resource, which I think can be very important for folks who know that they have an alteration in their normal DNA that has put them at risk for getting cancer is something called force. It’s an advocacy group with a lot of resources and it’s facing registry cancer, empowered or Force. If you look for that on the web, they’ve got a lot of information that could be useful from the standpoint of sort of precision oncology. I want to emphasize that the VA has actually become a leader in this area. I play some role in the VA. So this is a little self-serving, but the VA is actually one of the places where precision oncology is really being taken advantage of sequences as much more straightforward to get done.
FORCE – Facing Hereditary Cancer Empowered home page (facingourrisk.org)
Dr. Bruce Montgomery (51:23):
And there are quite a number of studies that are available through the VA. I think from the standpoint of, you know, for folks to be able to find the right information out there, the internet is a wonderful thing. In many regards. I think Dr. Pelman series here is probably one of the better sources. Be careful about what you find out there on the internet, because it isn’t curated and the information can be inaccurate at best. So taking advantage of your provider to help you to navigate resources, particularly with regards to research and sequencing and any other resources that they may be available may be able to make available to you is important. You may have had another specific idea in mind beyond just going to a major medical center in terms of resources.
Dr. Richard Pelman (52:16):
Well, the internet, like you said, has opened up a host of opportunities and some people take advantage of people with what they’re trying to sell. So again, I think using your provider to help you find legitimate pathways through the internet and, you know, the American Cancer Society, there are many of the NIH resources that you can find regarding your particular tumor. So in wrapping up, I’d like to always leave on a positive note while cancer is always scary. I can tell you personally that from where I started in medicine, beginning of a career to the end, it is a galactic difference. We have made huge strides
Dr. Bruce Montgomery (53:02):
Night and day, for sure, just in time. You and I have been in the field, you know, from 2004 to now, we went from having just hormone therapy to many, many different agents for prostate cancer and hundreds of agents for other malignancies, which are all improving outcomes for people. So more work is being done every day. I have a great deal of optimism just as you do that, now we’re going to get to the ultimate situation where we’re all out of business, which I wouldn’t be too sorry about.
Dr. Richard Pelman (53:32):
Well, Dr. Montgomery, I thank you. This has been just a packed informational session. So Dr. Montgomery, again, thank you so much, enlightening us regarding the advances in precision oncology.
Dr. Bruce Montgomery (53:48):
Thanks for all you’re doing to help folks to understand their risks, their health and their options. So thanks for all you’re doing. It was my privilege.
Outro (53:58):


